Poster Presentation 20th Lancefield International Symposium on Streptococci and Streptococcal Diseases 2017
Effect of influenza activity on the incidence and severity of invasive group A streptococcal disease: a retrospective study in England, 2008-2016. (#232)
An increase in invasive Group A streptococcal (iGAS) infections concurrent to the 2015/2016 influenza season was observed. We retrospectively assessed the impact of influenza on development of iGAS infection and fatal outcome, to inform future prevention strategies, by merging the laboratory confirmed influenza and iGAS infection databases using the unique patient identifier from 2008/2009 to 2015/2016 seasons (37th- 36th week). Influenza and iGAS coinfection was defined as the concurrent diagnosis within 15 days. All-cause case fatality rate (CFR) was calculated (within one week).
Overall, 44,429 influenza and 11,124 iGAS single infections and 111/55,553 (0.2%) co-infections were identified. Among coinfections, an increase of cases was observed 2015/2016 season (1.8%; 40/2,237) compared to other seasons (0.2%; p=0.0001 to 0.8%; p=0.04), and in 2010/2011 season (2.0%; 24/1,193); both dominated by influenza A(H1N1)pdm09. Irrespective to season emm1 was the predominant iGAS emm-type, following by emm89 and emm12. Influenza A/iGAS were most common coinfections (62.3%; 66/106), followed by influenza B (36.8%; 39/106).
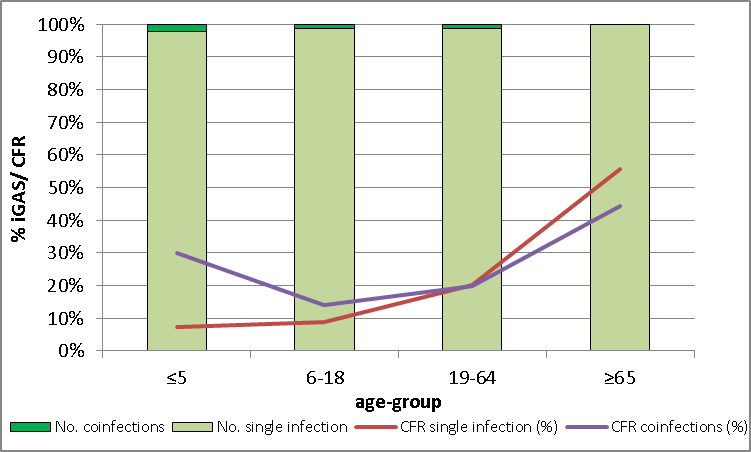
Overall, CFR was significantly higher among co-infections (22.6% vs 13.5%; p=0.006); particularly in the 2015/2016 season (27.5% vs 11.31; p=0.001). As shown in figure 1, CFR varied by age-group; among coinfections group CFR resulted higher in children ≤5 years.
This study identified an increase of influenza/iGAS co-infection in the 2015/2016 season, which was a late influenza season dominated by influenza A(H1N1)pdm09. Given the high CFR associated with co-infection especially in children, additional analysis aimed to clarify key factors in risk and severity of iGAS co-infection (such as influenza strain-type) are needed.